Formosa Plastics Explosion (2004) – Lessons in Operational Discipline
On March 23, 2004, at the Formosa Plastics PVC plant in Illiopolis, Illinois, a large release of vinyl chloride monomer ignited, causing a violent explosion. Five workers were killed and several others were seriously injured.
While many problems typically are present when an incident of this magnitude occurs, this incident is a powerful example of how failures in Operational Discipline — at both the organizational and personal levels — can lead to catastrophic loss of containment. In this case, an operator made an error, but rather than blaming the operator, a closer look at the CSB incident findings reveals why the operator might have acted as he did and how the incident could have been prevented.


What Happened
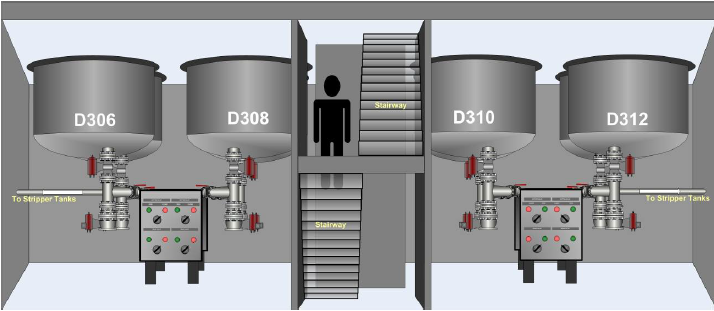
During a routine cleaning operation on a PVC reactor (D306), an operator mistakenly opened the nearby bottom valve of a polymerization reactor that was currently in operation (D310), apparently bypassing an active pressure interlock, instead of the bottom valve of the reactor that was being cleaned.
The contents of the operating reactor quickly filled the room, resulting in an explosion and fire that destroyed most of the reactor facility and adjacent warehouse.
As shown in the figure below, the reactors are near each other and have similar appearance.
CSB Incident Investigation Root Causes
The CSB investigation revealed that this was not an isolated event. The facility had experienced several previous incidents and near-misses involving similar procedural deviations. Process Hazard Analyses (PHAs) had also identified potential hazards related to reactor isolation, but the recommendations were not effectively implemented or tracked.
1. Borden Chemical (previous owner of the site) did not adequately address the potential for human error:
- Borden Chemical did not implement 1992 process hazard analysis (PHA) recommendations to change the reactor bottom valve interlock bypass to reduce potential misuse.
- In a 1999 PHA, Borden identified severe consequences for opening the reactor bottom valve on an operating reactor, but accepted the interlock, controlled by procedures and training, as a suitable safeguard.
2. Formosa-IL did not adequately address the potential for human error:
- After a 2003 incident at FPC USA’s Baton Rouge facility, Formosa-IL did not recognize that a similar incident could occur at the Illiopolis facility or take action to prevent it.
- Formosa-IL site management did not implement corrective actions identified in the investigation of a similar incident in February 2004 at Formosa-IL.
3. Formosa-IL relied on a written procedure to control a hazard with potentially catastrophic consequences.
OD Considerations
It is easy to blame the operator who bypassed procedures. However, the deeper and more important lessons lay in the organizational failures that allowed unsafe practices to become normalized.
- Organizational OD Failures: Management was apparently aware of repeated procedural shortcuts and previous incidents but failed to correct them in a timely way. PHA recommendations were not implemented or implemented quickly enough. Safe cleaning operations were dependent on procedures that had not been fully evaluated in PHAs, and the similarity of reactor design did not differentiate reactors easily, especially with most instrumentation in the upper control room. Leadership apparently did not establish clear expectations or accountability for following procedures.
- Personal OD Failures: Individual operators apparently routinely chose to bypass written procedures. Workers apparently did not speak up or stop work when they saw or were aware of unsafe practices. Awareness of the operating environment in this situation, while aggravated by lack of local instrumentation, was insufficient.
The Sherlock Holmes Lens
Applying the Sherlock Holmes mindset would have changed the outcome. Instead of accepting procedural deviations and previous near-misses as “normal,” a Sherlock approach would have treated every shortcut and earlier incident as a mystery worth solving. Key missed opportunities included failing to thoroughly investigate or follow-up on previous incidents and PHA findings, and not asking “Why are people consistently bypassing this step?” with enough rigor at the organizational level.
Key Lessons Learned
- OD has both organizational and personal dimensions — weak organizational OD is often a root cause that enables personal failures.
- A culture that tolerates shortcuts creates the conditions for potentially major incidents.
- Management must actively monitor and timely correct deviations rather than accepting them or appearing to endorse them.
- Strong OD and sensitivity to operations are essential for keeping hazardous materials “in the pipes.”
Call to Action
Review your site’s OD through the lens of the Formosa incident. If secretly surveyed, what percentage of personnel would say they always follow procedures as required without shortcuts? Are procedural deviations being tolerated? What systems are in place to catch and correct them?
What is one practical step your team could take to strengthen operational discipline?
- Download Case Study PDF
- CSB Video Animation of the Incident
- Is OD Your Greatest Opportunity for Improved Process Safety Performance?
- The Process Safety Professional as Sherlock Holmes